
Twitter photo by Rasu Shrestha MD, MBA, Chief Innovation Officer at UPMC
There are lots of ways to measure the success of a speech. One is what the audience says on Twitter during the talk. I’ll let them speak for themselves, below.
Power to the Patient!


Twitter photo by Rasu Shrestha MD, MBA, Chief Innovation Officer at UPMC
There are lots of ways to measure the success of a speech. One is what the audience says on Twitter during the talk. I’ll let them speak for themselves, below.
For the past several years a number of themes have repeatedly arisen in my work that aren’t widely discussed elsewhere, and I’ve wanted to make them available to wider audiences, so I’ve started recording occasional “slidecasts” – I play the slides on my computer and narrate. Here’s the latest. It’s a core topic in rethinking the patient-provider relationship: paternal caring, which is necessary in some situations, vs the increasing shift to patient empowerment, autonomy, and even emancipation – the removal of constraints.
I did this for my head & neck cancer patient friends in New Zealand, whom I met during my fellowship last fall. We’ve kept in touch on their Facebook group. On Thursday two of them, Maureen Jansen and Tammy von Keisenberg, are speaking about “health literacy” – a subject that’s misunderstood far too often, and which is often tied to discussions of whether patients should or can be independent to one extent or another. Food for thought.
Thanks once again to the sponsors and organizers of that fellowship: Spark Revera (New Zealand’s telecomms company, totally into the emerging world of e-health) especially @eHealthDoc Will Reedy MD, and Waitemata District Health Board, especially head & neck cancer surgeon David Grayson MD @Sasanof and its “i3” innovation center headed by Dr. Penny Andrew.
Email subscribers, to see the multimedia below, you may need to click the headline to view this online.
Last July I participated in a workshop on life after cancer at the National Academies of Sciences, Engineering, and Medicine in Washington. They’ve just published the final report, Long-term Survivorship Care after Cancer Treatment: Proceedings of a Workshop. It’s a free 160 page PDF.
 I keep seeing patterns of thought that I frankly think are pretty benighted. With luck, shedding some light on them will help. This one is so STUCK in darkness that I’ve decided to publish a little series on the subject.
I keep seeing patterns of thought that I frankly think are pretty benighted. With luck, shedding some light on them will help. This one is so STUCK in darkness that I’ve decided to publish a little series on the subject.
First is this editorial about patients in research. Next will be what happened when a researcher I know became a patient/family member. Then will be how this fits into a century-long timeline of progressing toward patient autonomy … which of course requires a matching increase in patient responsibility.
 To achieve its potential, healthcare must be democratized.
To achieve its potential, healthcare must be democratized.
I’ve reached this conclusion after hundreds of speaking events in eighteen countries over nine years. For me “speaking” has always involved a lot of listening and learning, and the more I’ve learned, the more I’ve puzzled over this paradox:

“Private suites. Caring staff. Room for family.” Woohoo!
On the way home last night I drove past this billboard, turned around, and went back to snap this photo. See, hospitals know that if we have a good maternity experience we’re more likely to come back when sick, so they offer this.
Fine with me, but when we DO come back, shouldn’t we get what they promoted?? Let’s ASK them to provide it, for ALL healthcare! Otherwise it’d be kind of a bait & switch, now wouldn’t it. :)
Empowered patients & families praise ’em when they do well, and when they don’t, we ask for what we need. Do it!
Edit: In a comment below, @MightyCasey points to another factor I should have noticed: while hospital marketing departments are promoting the service provided in their maternity suites, the grim reality remains that the US has the worst maternal mortality rates in the developed world. Here’s the chart from one of the NPR posts Casey links to, which uses data from a big (38 page) article in Lancet last year. Look at US healthcare’s performance in the past generation – this is the number of dead mothers per 100,000 live births; :
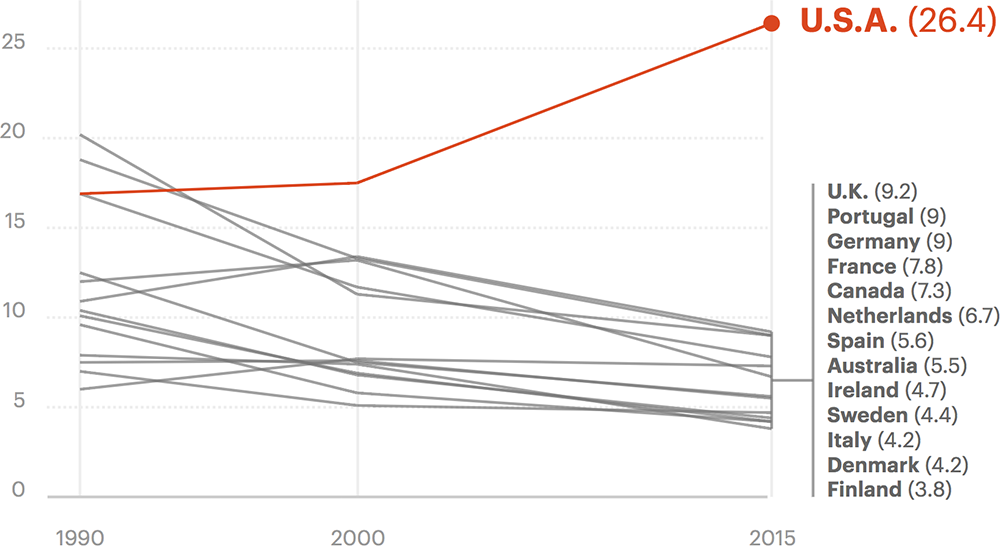
In short, while the marketing is ramping up, actual delivery of maternal care is getting much worse, especially compared to what other developed nations are doing.
China, for instance (not shown in this graph) has improved since 2000 from 85.2 maternal deaths to 17.7, while we’ve gone from 17.5 to 26.4. This matches my recent post on the e-patient blog about “amenable mortality,” which is whether a system actually delivers the care that it knows how to do.